CASE STUDY: FULL MOUTH REHABILITATION USING OUR DENTAL DS-EX Series SCANNERS
Case Profile
This patient was an 86-year-old woman. The patient had been treated several times in the past. In the early years, the mandibular posterior teeth were implanted, and the entire maxilla was reconstructed at an outside hospital(Fig 1, Fig 2). However, over time, due to unsealed and discolored bridges that caused aesthetic and functional discomfort, the metal-porcelain crown of the maxilla fractured, and had to be replaced (Fig 3)
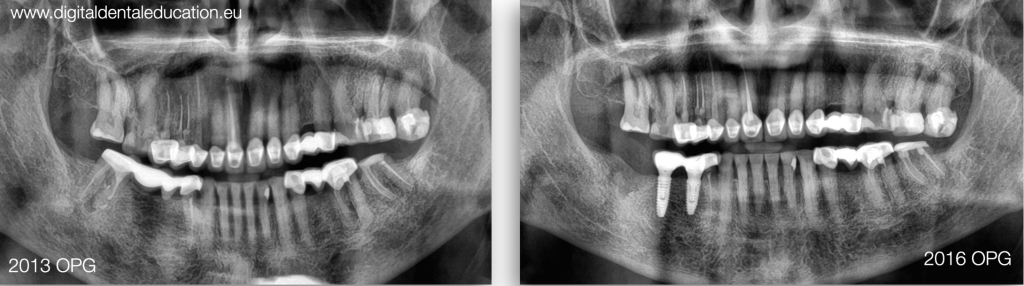
Fig 1: Implant restorations were performed at another hospital.
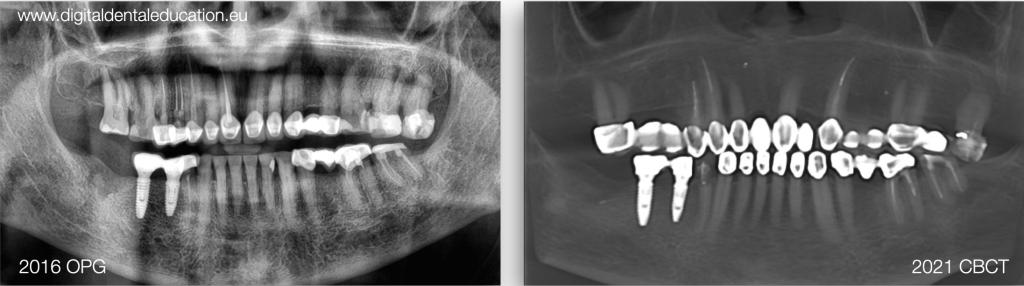
Fig 2: Full mouth rehabilitation was provided at another hospital.

Fig 3: The initial situation showed damaged upper PFM bridges that need to be replaced.
Diagnosis
Upon review, there are no TMD disorders, muscle pain, dysfunctional masticatory patterns, teeth grinding, aberrated smile line, group function, decreased OVD, or abrasion (Fig 4, Fig 5). The patient’s expectations were brighter color and greater exposure of the upper teeth while improving speech and masticatory performance with fixed prostheses. Because of the patient’s age, good adaptation and condition of lower restorations, the dentist decided to keep them as they were.
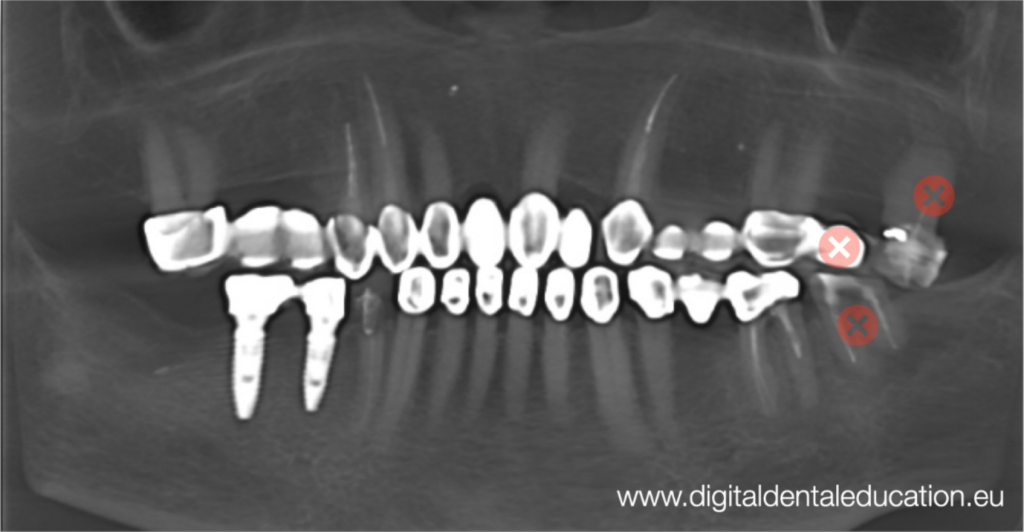
Fig 4: The functional and clinical examination
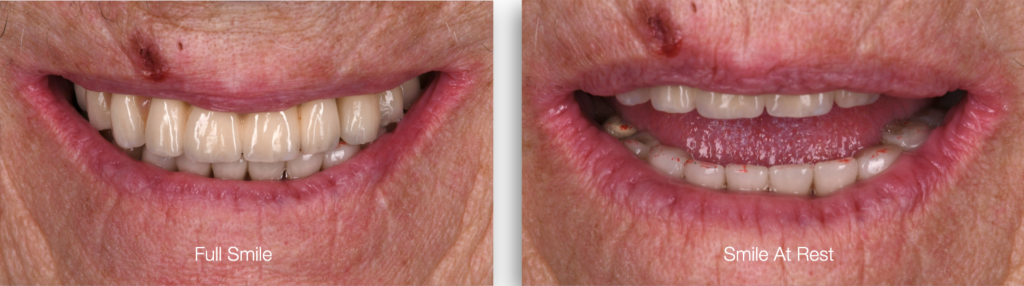
Fig 5: The Initial situation of full smile and smile at rest.
The DSD before treatment First, the dentist had taken some high-resolution photos of the patient and performed the DSD in dental software. After comprehensive communication, the patient was satisfied with the aesthetics of the tooth shape and the dentist proceeded with further treatment (Fig6, Fig7, Fig 8, Fig 9, Fig 10, Fig 11)

Fig6, Fig7, Fig 8, Fig 9, Fig 10, Fig 11: The digital smile design process.
Treatment process
The dentist removed the old bridge from the patient’s mouth, and fortunately there was a way to remove one of the bridges in one piece, moderate it, and use it as a long-term temporary until suitable gingival surfaces were formed for a proper pontic (Fig 12, Fig 13)

Fig 12: The long bridge taken off from the patient’s mouth.

Fig 13: The dentist made a little adjustment, removing some zirconia at the bottom of the bridge to make it suitable for long-term temporary use while waiting for the recovery of gingiva.
After three months of healing (Fig 14), the dentist refined tooth preparation and decided to take an intraoral scan for final restorations. He checked out the undercuts with an undercut tool (Fig 15, Fig 16, Fig 17, Fig 18), as well as provided photo and video procedures for smile design and proper virtual articulation positioning, which is a dentist’s original method called Photo-DFA Workflow.
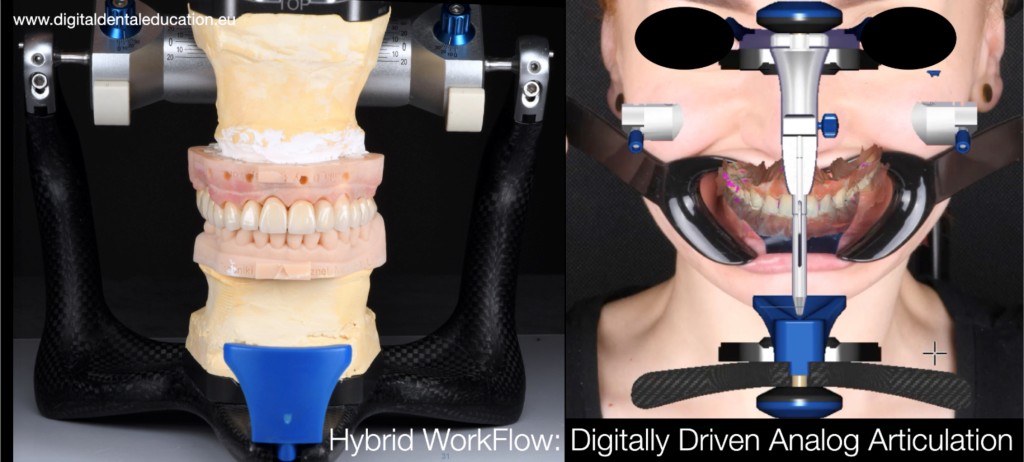
Fig 14: The gingiva was plump after three months.
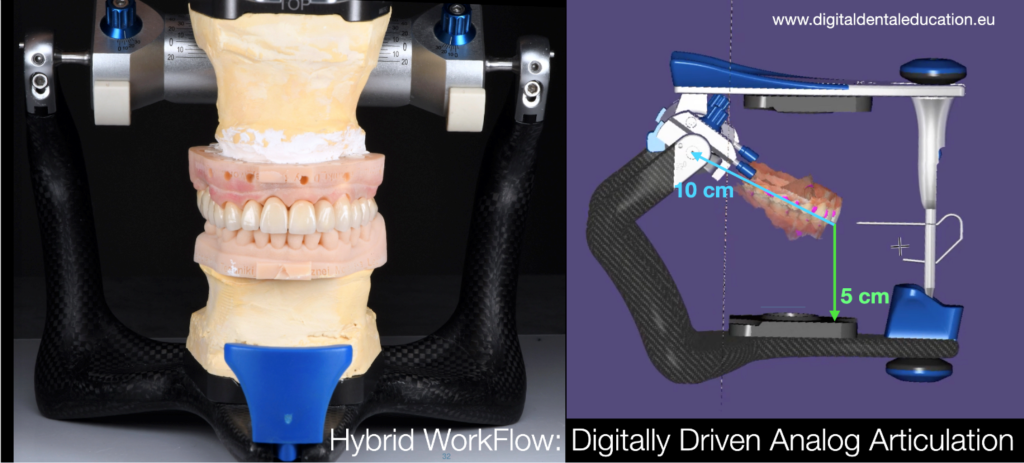
Fig 15: The scan data
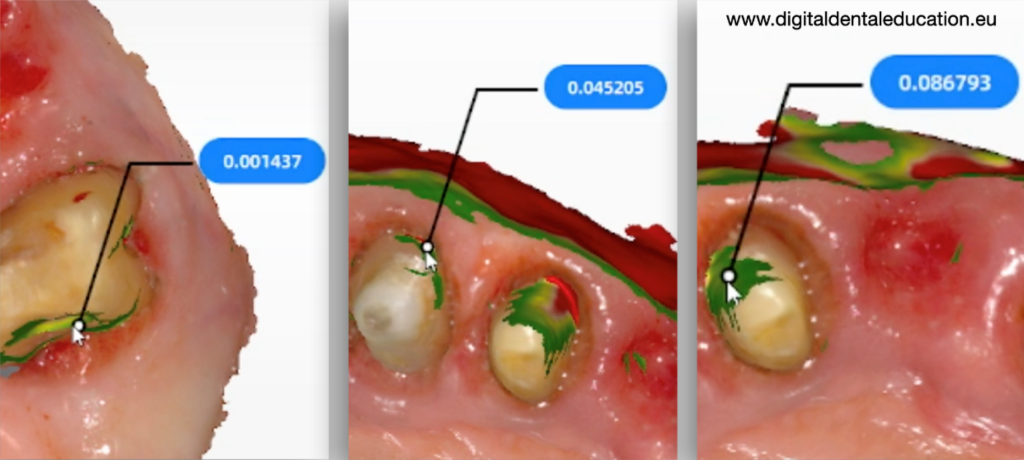
Fig 16: The undercuts were checked using the Intraoral scan software
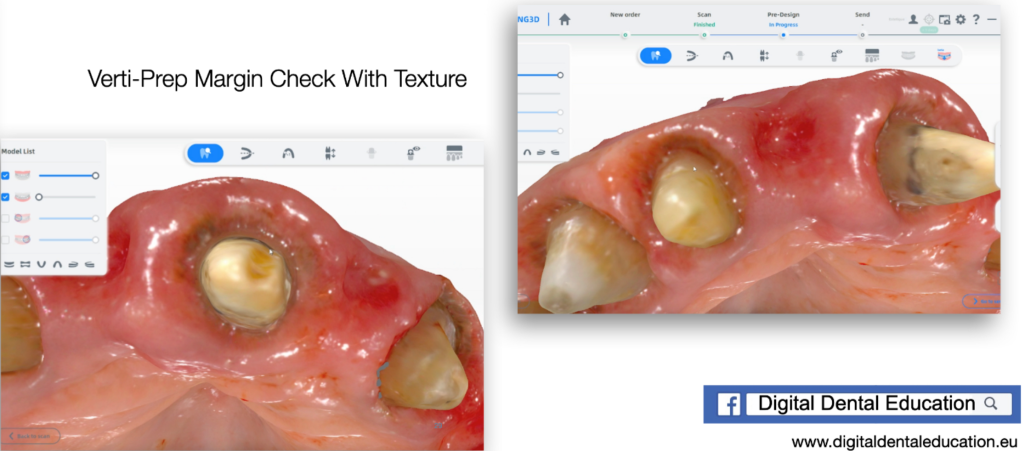
Fig 17: The checking process of the scan data, it showed a clear margin line on the digital model.

Fig 18: The occlusion situation after tooth preparation.
This method combines two concepts together, facebow concept for esthetic and functional inclination setup and DFA for rotation axis positioning. By using a certainly inclined portrait photo of the patient, the dentist had developed a procedure of aligning the 3D intraoral scan over the 2D photo, and by using Kois DFA articulation rules they can achieve a proper position of the scan inside the virtual articulator (Fig 19, Fig 20).
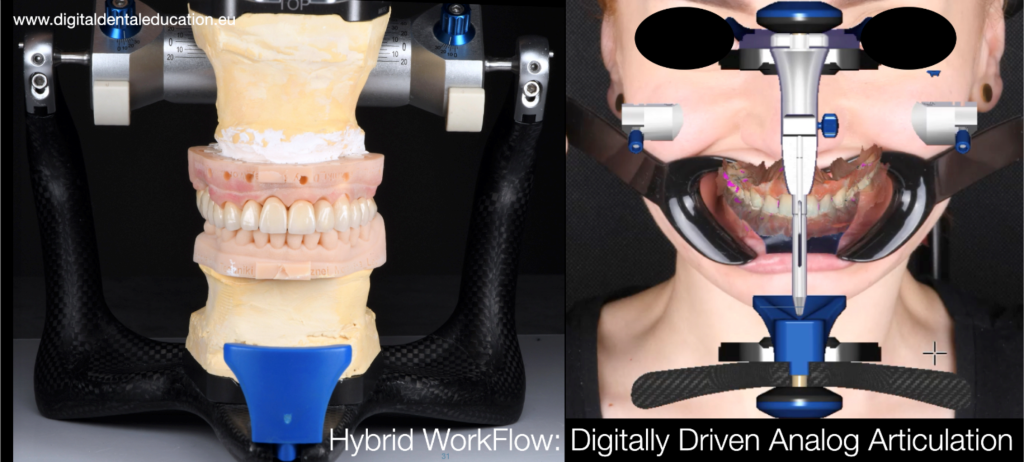
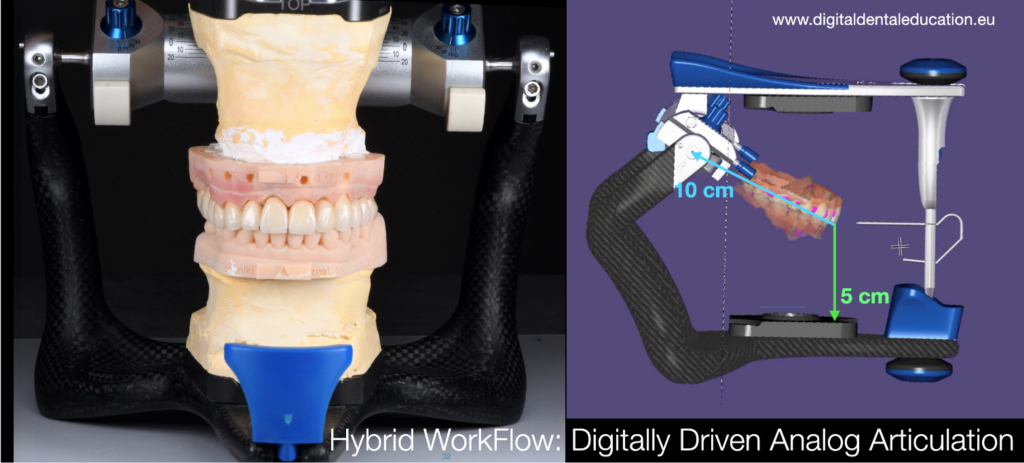
Fig 19, Fig 20: The Photo-DFA Workflow invented by the dentist.
The scan data was sent to a 3D printer for printing, and with the smile design confirmed by the patient, the dentist created the final porcelain multilayered zirconia bridges. It fitted well with the printed model (Fig 21, Fig 22, Fig 23, Fig 24).

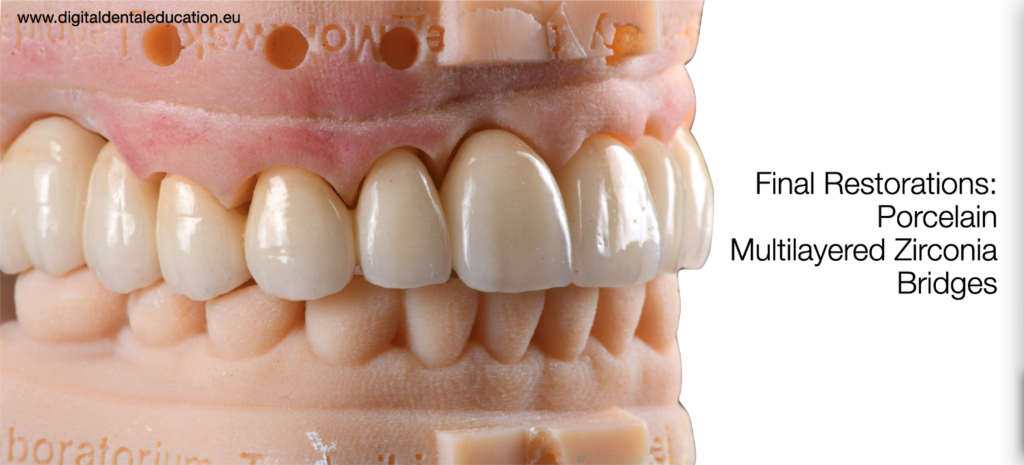

Fig 21, Fig 22, Fig 23, Fig 24: The long bridges fitted well in printed models.
The final restorations cemented into the mouth



Fig 25, Fig 26, Fig 27: The final restorations fixed in patient’s mouth.

Fig 28: The smile before and after treatment
The dentist’s comments
Aoralscan3 was an important scanner used for this case. We can complete the scan in one minute, and the high precision and accuracy are critical for bridges with large spans to avoid complications such as zirconia fracture, cracks and spalling.
This approach helps reduce the number of appointments, which are usually reduced to 3 total – 1. preparation; 2. try-in (not always, usually patients accept their new teeth at try-in so we can cement them immediately); and 3. final delivery. Of course, there may be an additional appointment for the final adjustment and close inspection and checkup.
About dentist Pawel Szuba-Paszkiewicz

Fig 29
Pawel Szuba-Paszkiewicz graduated with honors from the Faculty of Dentistry at the Medical University in Wroclaw in 2004. Pawel Szuba-Paszkiewicz performs treatments of complex medical procedures in the field of CAD /CAM prosthetics, implant prosthetics, full-mouth rehabilitation and minimally invasive esthetic dentistry. Nowadays, his professional interest is focused on digital prosthodontics and implant prosthetics with its complete digital workflow. He has developed and introduced his own innovative procedure of tissue retraction during digital prosthetic procedures, the Endo-Resto Single Visit Chairside Restoring Workflow, as well as the innovative, fast and complex Smile Design & Delivering Protocol (SDDP), “Photo-DFA” workflow. (Fig 29).






















Leave a comment